
The views in this article are entirely my own and do not reflect that of any organisation I work with. They should be considered reflective of my position at the time of writing, which may have since changed.
The National Institute for Clinical Excellence (NICE) has released its guidelines for critical care in Coronavirus. NICE is widely respected, and its evidence-based guidelines often take years to develop, with wrangling backwards and forwards between medication companies, researchers, journal articles etc. The fact that it’s provided guidelines so quickly in the case of coronavirus is impressive. BUT NOT THE CONTENTS
There has been discussion in the press for a while about moving to limit access to critical care for people deemed most likely to benefit from it – e.g. most likely to survive, maybe with an element of assessment of quality of life in there. In the press, some people have proposed limiting it to people below a certain age (below 60 and below 70 are both mooted), probably on the ethical basis that those people have fewer years of life ahead of them than younger people can be presumed to, and thus that there would probably be fewer years of life saved by treating them compared to someone younger.
Better that an official guideline is made than that decisions are made on a case by case basis, but the ethical basis of the guideline is what’s difficult to decide. Under the UK guidelines:
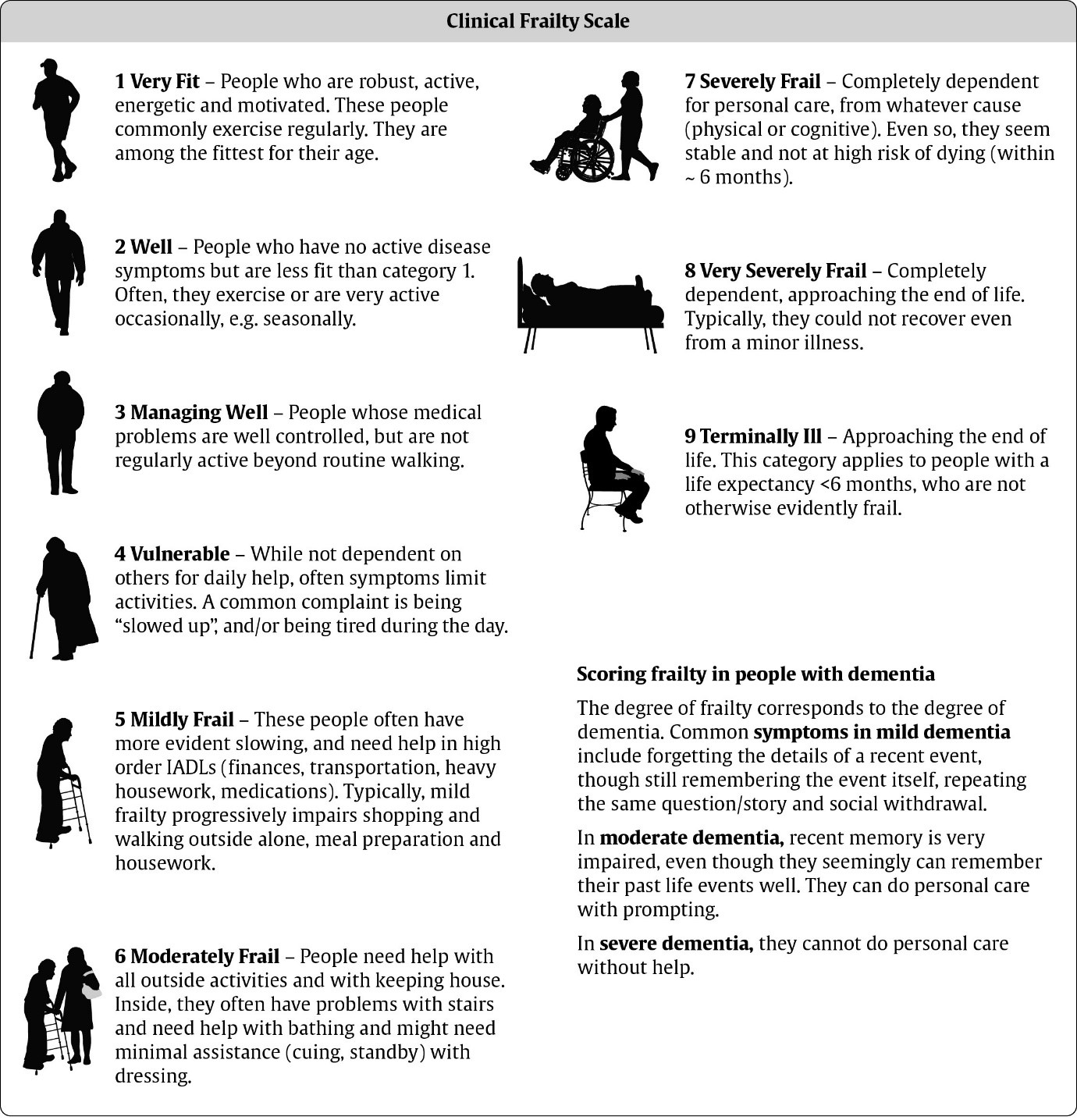
- On admission to hospital, a patient’s clinical frailty scale (CFS) is calculated
- If the patient needs critical care, and this is below 5, and the patient is likely to benefit from critical care, then they are typically admitted
- If this is above 5, or there is uncertainty about the benefit, then their case is discussed with the critical care team
- Health professionals are asked to discuss treatment plans with people who would not benefit from critical care or who don’t wish to be admitted
- Health professionals are asked to discuss a Do Not Attempt CPR decision with people with capacity and a CFS score of 5 or above
- If critical care is started, it should be stopped if it seems less realistic for the goals of critical care to be achieved
{kind=link}
The Clinical Frailty Scale looks at the amount of support people need in their daily lives and uses this as a proxy for likelihood to respond to treatment. This is a dangerous scale to use because what it measures is not level of illness but degree of support needed in your daily life. I score 7, which is the highest score given to people who are stable and not expected to die in the next 6 months. To score below 5, you need to be independent, and not requiring support. You might be “slowed up or tired during the day”, but you don’t need help with any activities of daily living, including heavy housework.
Once you start to need help with housework, that’s it – you’re no longer an automatic ‘in’ for critical care treatment. If. like me, you’re reliant on someone for all aspects of personal care, then however stable your health is, and however likely you are to survive coronavirus, you’re likely, especially as the crisis builds to not be given treatment.
The Clinical Frailty Scale doesn’t seem designed for younger people. A brief bit of research only suggests that it’s been used and validated on a geriatric population. This means that while it may be accurate in predicting outcomes for elderly patients, it has not been proven to be an accurate predictor for younger people. As frailty syndromes with elderly people are a result of all the aspects of the body and mind slowly becoming worn out, if someone hits a certain score on the scale, this would indicate something about their overall health state and hence predict outcomes. For younger people, who might need social care for reasons that don’t affect their likelihood to survive coronavirus, decisions will be made about us without questioning us.
For younger people who need help with activities of daily living, there seems to be no evidence that the scale is accurate in predicting our outcomes. It makes the assumption that needing full support with personal care means someone is less likely to survive Coronavirus, and then, by allocating treatment to them on that basis, makes them less likely to survive treatment by deprioritising them for it. Applying this scale to our lives is therefore dangerous and highly concerning. We will be considered low priority for treatment and then killed, without any real assessment of whether we would have survived it.
The NICE guidelines also make reference to providing treatment as long as people will recover to an extent that is acceptable to them, but make no attempt to find out what extent is acceptable to people. This runs the risk of doctors predicting that someone would have a low quality of life if, for example, given a tracheostomy and ventilator for the rest of their life, when actually that outcome might be acceptable to them – it would to me.
Obviously decisions have to be made about who to treat, and how. It is a reasonable outcome commensurate with the general NICE attempts to maximise quality adjusted life years (years of expected life gain at full quality of health). Many disabled activists oppose this, arguing that the arbitrary decisions made are based on assumptions of our health state and what people who are themselves well presume our quality of life will be. This is often underestimated by people who are not disabled.
The application of a measure to young people to determine the treatment we will be given if we need critical care, which as far as I can tell has not been validated in our situation, is incredibly dangerous. This will lead to a disproportionate number of disabled people who would have had every chance of survival instead dying of coronavirus unnecessarily. The CFS will not adequately identify our chances of survival, and its application will be fatal.